Find advice on a range of topics to help you live life to the full, from diet and exercise to travel, work, sleep, relationships and leisure activities.
Our interactive Parkinson's map shows a range of resources across Europe, from member organisations to events, activity groups to research and campaigns
Cure Parkinson’s is calling for fundraisers to embark on walking challenges to raise money and awareness for Parkinson’s. It comes as the research charity marks its 20th anniversary.
The bid follows in the footsteps of the charity’s co-founder, the late Tom Isaacs. The campaigner undertook a year-long walk around the 4,500 mile coastline of Britain in 2002.
The charity was set up in 2005 by four people living with Parkinson’s who wanted to see a Parkinson’s cure taken more seriously. It has since funded millions of pounds of research, including directly funding 13 clinical research trials.
Cure Parkinson’s Chief Executive Office Helen Matthews says: “This year we are encouraging our supporters to get involved with Cure Parkinson’s by walking, celebrating our late co-founder Tom Isaacs’ epic walk around the coastline of Britain.
Photo credit: Philip Brown
“Our aim is to cure Parkinson’s and the only way we will do this is through the help of all our incredible supporters. We would be so thrilled if you would join us.”
Cure Parkinson’s fundraiser and person with Parkinson’s Sally Franck has raised more than £30,000 for Parkinson’s charities. Her walking challenges have included Hadrian’s Wall, Offa’s Dyke, and more recently Alfred Wainwright’s Coast to Coast.
“Walking brings so much pleasure, whatever distance you can manage. It might be just walking 100 metres up the road or taking on a long distance trail – but the challenge is there and the benefits from achievement are plenty,” she says.
“There is no cure for Parkinson’s and that makes it a life sentence not only for us, but also for all of those who live with, love and look after us. I know that what we all need is some hope; hope that a cure can be found as quickly as possible.”
Support for Cure Parkinson’s vision
Dominic Graham, Parkinson’s Europe’s Operations Director, praises the campaign. He says: “Tom Isaacs was a visionary co-founder of Cure Parkinson’s. He was also a dear friend of Parkinson’s Europe, and a highly valued Board member back in the 2000s.
“His relentless spirit and unwavering commitment to finding a cure profoundly inspired us in our own mission. We miss him greatly, and are proud to support this campaign. It so beautifully honours his pioneering legacy and continues the vital work he started. We will continue fighting alongside his vision for a world free of Parkinson’s.”
Supporters can organise their own walking fundraiser, or take part in Cure Parkinson’s organised walk in London on 28 September.
UK-based organisation Cure Parkinson’s has launched a £2 million funding call to test rationally designed combination therapies for disease modification...
Meet Parkinson’s Europe’s new Empowerment Steering Group
Meet the team who will support our work to build knowledge, connect Parkinson’s communities with each other and other stakeholders, and boost communication with healthcare professionals
A Parkinson’s nurse, physiotherapist and Deep Brain Stimulation patient are among those who have joined together to form Parkinson’s Europe’s new Empowerment Steering Group.
The second of three new steering groups has been set up to guide and support the empowerment pillar of the European charity’s new strategy.
The work aims to build knowledge, understanding and capacity of national associations and groups. It intends to connect Parkinson’s communities with both each other and other bodies such as the treatment industry. It also hopes to boost communication and understanding between people affected by Parkinson’s and healthcare professionals.
The new Steering Group held its first bimonthly meeting in May, overseen by the Outreach and Engagement Manager Jessie Duncan and the Strategic Director Amelia Hursey.
“We are very excited to see the enthusiasm, passion and skill that our members in the Empowerment Steering Group collectively have,” says Amelia. “With their help, we will make sure all of our activities that fall under our empowerment pillar will be focused, relevant and fit for purpose for our whole community.”
Meet Parkinson’s Europe’s Empowerment Steering Group members:
Ellen Causin is a French-Australian physiotherapist with experience of living and working in Australia, the UK, and France
“I am passionate about empowering people with Parkinson’s, as well as the health professionals who support them, through knowledge sharing. I believe this empowerment group will be a fantastic way to help achieve that goal.”
Friedhelm Chmell has many years of experience in Parkinson’s care, and now works as a Parkinson’s Nurse
“I believe that after more than 22 years in the care and counselling of people with Parkinson’s, I can contribute to strengthening the Parkinson’s community in this way. And at the same time, I am always interested in learning from others.”
Janette Sinclair is British, and lives in Brussels, Belgium. She has had Parkinson’s since 2013 and had Deep Brain Stimulation surgery in January 2025
“I am interested in bringing together and helping people with Parkinson’s to take control of their lives. From the outset after my diagnosis, I have been an advocate of intensive sports and physical activity for people with Parkinson’s.
“I have been involved in developing this at a local level through Action Parkinson, a Brussels-based activity centre for people with Parkinson’s. I am currently a board member of Action Parkinson’s and of Parkinson’s Europe.”
Jagoda Machajek works at the Brain Disease Foundation
She is responsible for communication, creating and coordinating projects, and sharing her personal experience with patients who reach out for information.
“I want to share my experience primarily from the perspective of a caregiver for my mother – the founder of The Brain Disease Foundation in Poland.”
Marco Ramelli lives in Florence, Italy, and was diagnosed with Parkinson’s 13 years ago
“We must spend our time better, making sure life includes important things like diet, good habits and doing what you love to do. We need research. Research could give us new weapons, new possibilities, new lifestyles.”
Matthew May is a chemist-turned-medicines-developer and lives in Switzerland
He works for pharmaceutical company Roche but has previously worked at non-profit organisations.
“I love working at the interface of where science meets people. Since finding out as a child that my grandfather had Parkinson’s, I have wanted answers and solutions. I then worked at DIA and the European Patients Forum, and I helped set up the European Patients Academy which helped others learn about medicines development. This is something I am passionate about continuing, even if I now have another job.”
Peter DiBiaso is a Parkinson’s advocate and life sciences professional, committed to finding a cure for Parkinson’s
“I was diagnosed with early onset Parkinson’s nearly 10 years ago, and I am particularly committed to promoting awareness and participation in clinical research trials. I am most interested in the ability to build bridges across our patient advocacy communities, whilst enabling global support through continued engagement and collaboration.”
ZWAP Co-Founder Rune Vethe lives in Sandefjord, Norway, and was diagnosed with young-onset Parkinson’s 16 years ago
“I enjoy being part of both the local, national and international Parkinson’s community. I believe in the importance of a European umbrella organisation and would like to be involved and try to contribute.”
Lucia Power lives in Ireland and has worked in the health and social care sector for 29 years.
“I have played a key leadership role in the development of disability and neuro rehabilitation services in Ireland both at service and funded level. I currently have a management role in the regulation of social care services.
“As a person with Early onset Parkinson’s, I have never let the condition define who I am, I believe in putting the ‘person’ first and that any intervention is about supporting the person and their uniqueness.”
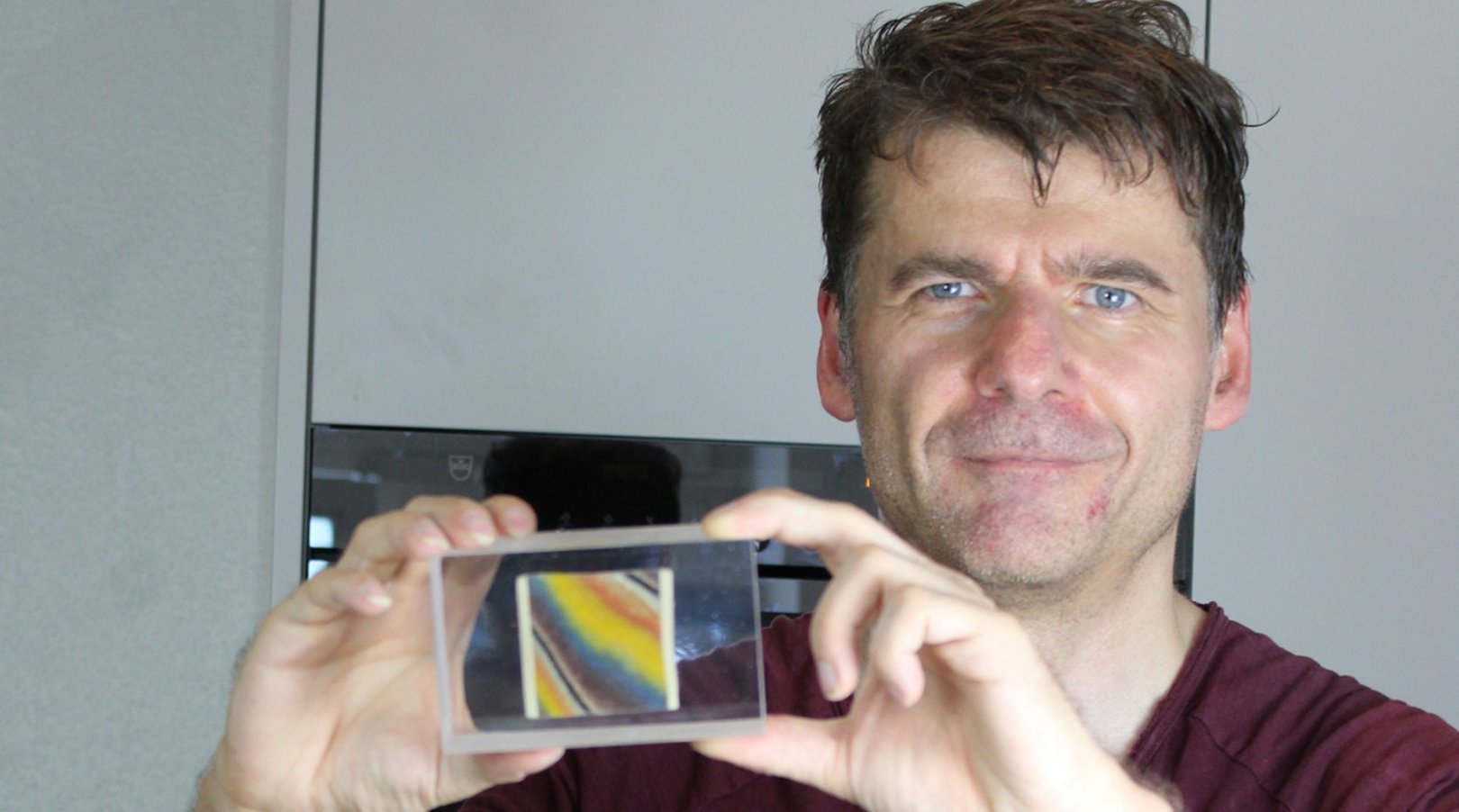
Creating intricately detailed pieces of art from pasta may not be the skill you would expect from a software engineer with early-onset Parkinson’s. Albeit one living in a picturesque town near art-rich Basel, the culture capital of Switzerland. But to 56-year-old Urs Bratschi, it is as natural a pairing as spaghetti and tomato sauce.
“Both professions demand creativity, and I find fulfillment in balancing the structured logic of software engineering with the expressive freedom of art,” he tells Parkinson’s Life.
It has been two years since Parkinson’s Life last spoke to Urs, when he was showcasing his early pasta artworks at his first exhibition. His art has greatly evolved in that time, he tells us, using his skills to not only share the techniques with others but to also open up conversations about his Parkinson’s journey.
“I discovered joy in explaining my creative process to others—how I craft, preserve, and encase pasta in resin. Given the connection between my art and my Parkinson’s diagnosis, discussions often touch upon the disease,” he explains.
“While many are hesitant to broach the topic, I approach it openly, aiming to inform without seeking pity. I prefer my art to stand on its own merit.”
Honing his craft has seen Urs explore new methods and styles, creating even more intricate images composed of multiple pasta elements, along with bowls and plates filled with various pasta types set in resin.
“I have essentially pioneered a new art form,” he explains. “However, many art enthusiasts and gallery curators struggle to categorise it, necessitating efforts to raise awareness.”
These efforts are paying off, with Urs taking part in 12 art exhibitions last year, in locations from London to Luxembourg, and Germany.
Pasta and Parkinson’s: a rich and fulfilling life
Likening each of his artworks to being “like a child” to him, Urs’ passion for his creative works is evident – and inspiring. More than a hobby, it is part of his drive to show that a life with Parkinson’s can still be rich and fulfilling.
“I am active in a support group for young Parkinson’s patients, sharing my experiences and journey,” he says. “Initially, some find it hard to believe when I say that many positive aspects have emerged from my diagnosis, making my life more exciting and meaningful. But living this truth lends it credibility.”
Last November, he appeared on Swiss television in a health program discussing life with Parkinson’s, and has also co-authored a book exploring art in the context of neurodegenerative diseases. “I delve into the question, ‘Why do I have Parkinson’s?’—a question I answer by the chapter’s end,” he says.
Accepting a life-changing diagnosis
This positive mindset was – understandably – not Urs’ first response to learning of his Parkinson’s diagnosis in 2014, at the age of 45.
“Upon receiving the diagnosis, my world collapsed,” he says. “I trembled uncontrollably – not due to Parkinson’s – and could not work. I often sat at my desk, overwhelmed with tears. Suicidal thoughts emerged, leading me to seek psychiatric help.”
Helping Urs climb out of that “abyss” took a team of friends and healthcare professionals who provided “immense support”, along with his belief that giving up was not an option. “A pivotal, albeit harsh, realisation was accepting that no one could cure me; Parkinson’s was here to stay.”
Once he accepted the diagnosis, he felt able to explore the condition, and even begin to consider a more positive approach. “For the first time, I seriously contemplated my life’s direction and aspirations. My perspectives shifted; some things lost importance, while others gained significance. Overcoming such a profound upheaval has been an invaluable experience, propelling me into unimaginable dimensions.
“This disease awakened me. I now internalise the belief that we have one life, and it is up to us to make it meaningful. Parkinson’s has become a driving force, motivating me to achieve. I’ve befriended my illness—it’s part of me, and I of it. I firmly believe that a positive attitude can influence the disease’s progression. Ten years post-diagnosis, I feel well and content with my life.”
An evolved worldview
As a gay man, embracing change and evolving his perspective is not totally new to Urs. “Before realizing I was gay, I knew little about it and held rather negative views,” he says. “Accepting and embracing my sexuality was challenging—I did not want to be gay. This reinforces my belief that it’s not a choice; it is inherently part of us.”
Looking back, Urs can draw parallels between the two parts of his identity, as well as key differences. As with Parkinson’s, coming to terms with his sexuality turned his “world upside down” and challenged him to adjust his perspective on life, Urs says.
However, he adds: “Unlike Parkinson’s, being gay isn’t inherently problematic—unless one lives in a society that persecutes or marginalises LGBTQ+ individuals. Nonetheless, I had to work on myself, and reshape my worldview. Both journeys expanded my horizons and opened my heart. The Parkinson’s diagnosis came about 20 years later.
Having previously navigated such a life-altering realization perhaps equipped me better to handle this disease. Often, it is the negative experiences that teach us the most. Today, I live happily as a gay man and would not change that. I also live contentedly with Parkinson’s, though I would gladly part with it if I could.”
While research suggests challenges facing people in the LGBTQ+ Parkinson’s community can include discrimination in healthcare, a lack of recorded data around gender identity and the need for best practice guidelines and inclusive support groups, Urs says he has had a positive experience to date.
“In Switzerland, LGBTQ+ individuals are largely accepted and integrated, though rural areas might be slightly less progressive. I have never felt discriminated against when seeking medical care,” he says.
“My artistic endeavours even pique the interest of neurologists. For instance, the University Hospital in Bern produced a video about me, highlighting the intersection of art and Parkinson’s.”
He also participated in an exhibition organised by the University Hospital in Zurich last year, featuring artists with Parkinson’s.
Collaboration and community
Along with cultivating a positive mindset, building good relationships is another part of Urs’ approach to living well with Parkinson’s. This includes being part of a “wonderful” support group for young people with Parkinson’s patients, and maintaining a good relationship with Parkinson Switzerland.
“Interacting with fellow ‘Parkis’ is often special,” he says. “Even without knowing each other well, there is a deep sense of understanding and empathy. I speak very openly about deeply personal things. But that didn’t come naturally. I didn’t grow up in a family where people talked openly about feelings or problems—I had to learn that myself.”
In the future, he hopes to also see improved collaboration between conventional and alternative medicine. “Often, there’s mutual misunderstanding. However, from a patient’s perspective, there’s a significant demand to integrate both approaches.”
Urs Bratschi’s pasta art for beginners:
Interested in having a go at pasta art? Urs’ impressive creations are the results of years of experience, but he has set out a simple guide below for budding pasta artists to try it out.
Starting with stripes is the simplest. Lay alternating colored strips on an uncolored dough sheet (a tagliatelle cutter can help), then roll it out again
This technique allows you to craft ravioli, tortelloni, rigatoni, or penne with striped patterns.
To colour your dough, vegetable powders are effective. With the popularity of smoothies, powders like spinach or beetroot are more readily available and can be mixed into the flour during dough preparation
With summer just around the corner, and the new-look Parkinson’s Passport available in multiple languages, it is a great time to plan a break. Parkinson’s Life spoke to author and campaigner Timo Montonen to hear his top tips for travelling with Parkinson’s.
Travel tips for people with Parkinson’s
“Like hundreds of other people with Parkinson’s, I planned to attend the fourth World Parkinson Congress (WPC) in Portland. But living in Finland, I was faced with a long-distance trip across the Atlantic to the US – which I decided would be better with a team of friends. Besides, it’s more fun, safer and cheaper to travel in a group.
“We travelled by planes and vans to the west coast, visiting San Francisco, Los Angeles and Las Vegas on the way to Portland. The two-week journey was a success and we discussed afterwards what we could have done to make it even better. As a result, we created the following list of advice for other groups of people with Parkinson’s who wish to travel.
Plan ahead
“Start planning well before the trip to avoid stressful situations. Decide everyone’s role in advance – in particular, who will be group leader. The schedule must be arranged according to the slowest member of the group. Keep the budget clearly in mind and follow it. Research the different ways to travel as a group. Assess the pros and cons of using different vehicles such as aeroplane, train, ship, coach and minivan.
Manage your medication
“Make sure that you have all the medication that you need for the journey – and also take enough for a few extra days in case of delays. Take care of the medication schedule. Put prescriptions, and all other documents – such as a ‘Parkinson’s Passport’ – necessary for travelling, in one folder to make them easy to find when needed.
Prepare for the airport
“If you have deep brain stimulation equipment, artificial joints or pacemakers, take all documentation with you so that you can inform staff at the airport. Internal metal plates can be detected by body scanners at security checks – be ready to explain any medical implants to security staff.
Pack light but include key tools
“Always remember to pack your essentials, but try and travel light. If you use a seat cushion, pack it in your cabin bag along with the other things that you’ll need during the flight. Eating while on the plane is easier if you bring your own spoon and non-slip mat that you can place under your plate. Take straws with you to help with drinking, and extra napkins for any accidental spillages, as the plane does not always have them. Ankle supports, a back support and a seat cushion will all help tired muscles.
Dress comfortably
“Dress comfortably in loose clothing. Wear support stockings to prevent the lower legs from swelling. Take comfortable shoes that are easy to put on and take off. Bring warm socks or slippers on the plane with you to wear when walking up and down the aisle for loo breaks.
Timo Montonen and team.
Queue jump
“Inform the airport check-in staff and the plane personnel about the condition of your group – that you cannot stand for a long time in queues, for example. It’s possible that you may be able to ‘fast-track’ your way to the front of queues. If you use walking aids and/or wheelchairs contact your travel agency or flight operator in advance to ask for extra assistance at the airport.
Move mindfully on the plane
“Remember to stand up and stretch regularly while on the flight – bend the knees, stretch your legs, rotate your ankles, stretch your back, bend your upper body from side to side, raise your hands above your head. When it’s time to leave the plane remain, in your seat until the plane is almost empty – it’s no fun to stand and wait in a crowd.
Meal plan carefully
“Try to eat breakfast in your usual manner. When the group is on the road, having lunch can take a surprisingly long time, as you have to find a restaurant, order, eat and get the bill. To save time, eat a packed lunch during the day and have a sit down dinner in the evening.
Have a flexible itinerary
“Start mornings in peace. Remember to take rest breaks during the day. If the group is lacking energy, leave something out of the schedule to focus on the most important or most comfortable option. It’s OK to take a day off from the planned itinerary if the group could benefit from a rest day.
Take care of the team
“Take care of all members of the group. Make sure that all are able to cope with the schedule. Work creatively according to the situation, but don’t assume that all will follow the plan. Don’t leave anyone alone. Make sure you’re prepared if there is an emergency. Remember, worrying too much about Parkinson’s disease will not help you or your team.
Above all, enjoy the trip!”
Timo Montonen and team at the World Parkinson Congress, September 2016.
“Een off-periode is gewoon ontzettend vervelend!” zegt Gary Boyle, bestuurslid bij Parkinson’s Europe, die in 2011 de diagnose Parkinson kreeg.
Een off-periode bij de ziekte van Parkinson doet zich voor wanneer de medicatie van iemand met Parkinson uitgewerkt raakt.
“Het is zowel een motorisch als een niet-motorisch fenomeen, dus ongeacht hun motorisch profiel en hun niet-motorisch profiel kunnen deze symptomen verergeren,” vertelt Brian Magennis, verpleegkundig specialist in het Mater Hospital in Dublin en bestuurslid bij Parkinson’s Europe. “Als hun medicatie uitgewerkt raakt, kunnen ze ook non-motorische symptomen krijgen, zoals gevoelloosheid, tintelingen, een vreemd gevoel in de buik, een opgejaagd gevoel, irritatie, een slecht humeur, slapende lichaamsdelen – allerlei vreemde, vervelende symptomen – en zodra de volgende dosis begint te werken, stoppen ze weer.”
In het algemeen beginnen off-periodes als iemand ongeveer tien jaar Parkinson heeft. Iedereen ervaart Parkinson anders en dus zijn off-periodes ook voor elke persoon anders.
Gary legt uit hoe zijn off-periodes verlopen. “Het begint bij mij met trillingen in mijn hand en in mijn arm. Ik beweeg veel langzamer. Ik kan niet goed schrijven. Het is moeilijk om mijn telefoon te gebruiken. Ik voel me somber, ik ben nerveus. En ik vraag me af wanneer de off-periode weer over zal zijn. Off-periodes hebben een enorme impact op bijna alles.”
Het woord ‘off’ suggereert dat iemand plotseling heel hard achteruit gaat, maar het kan ook een geleidelijk proces zijn.
Omgeving en levensstijl, zoals eetpatroon, voeding, beweging en slaap, en ook het moment van de dag hebben allemaal een impact op iemands off-symptomen. Off-periodes kunnen zich zowel ‘s avonds als overdag voordoen. En ze kunnen ook plotseling en schijnbaar zonder reden gebeuren.
“Plotselinge off-periodes komen zelden voor maar als ze gebeuren, zijn ze heel slopend,” vertelt Gary. “Mijn off-periodes hebben nooit langer dan vier uur geduurd – dat was de langste – maar gebeuren wel bijna elke zes maanden en vaak op momenten dat ik het niet verwacht.”
Als iemand ineens meer off-periodes heeft dan normaal – binnen een aantal dagen of weken – heeft dat volgens Brian meestal een reden. Het is meestal een tijdelijke achteruitgang en betekent niet noodzakelijk dat uw Parkinson erger wordt. Maar het is belangrijk om contact op te nemen met uw zorgverlener, die u kan helpen om de oorzaak te achterhalen.
In de meeste gevallen heeft een plotselinge toename van het aantal off-periodes een van de volgende 10 oorzaken:
U hebt last van constipatie. Hierdoor worden Parkinson-medicijnen minder goed door het lichaam opgenomen en zijn ze minder effectief.
U bent ziek (u hebt bijvoorbeeld een urineweg- of luchtweginfectie, of griep) of u bent herstellende van een operatie. Dit belast het lichaam en kan ervoor zorgen dat uw symptomen tijdelijk verergeren.
U zit in een periode van stress.
U bent uitgedroogd. Hierdoor neemt het bloedvolume af, waardoor medicijnen minder goed worden opgenomen.
U neemt uw medicatie op de verkeerde tijdstippen of uw medicatieregime is veranderd.
U neemt medicijnen met een contra-indicatie voor een ander gezondheidsprobleem dan uw Parkinson, waardoor uw Parkinson-medicijnen minder effectief zijn.
U bent depressief. Uw motorische en niet-motorische symptomen kunnen hierdoor verergeren.
U hebt acute of chronische pijn.
U bent angstig of hebt paniekaanvallen. Hierdoor kunnen uw motorische symptomen toenemen. Angst is ook een veelvoorkomend symptoom als de werking van een dosis Levodopa afneemt.
U slaapt slecht. Wanneer u langere tijd niet goed slaapt, kunnen motorische functies (tijdelijk) verslechteren.
“Constipatie is een belangrijke factor, want dat voorkomt dat Levodopa wordt opgenomen,” vertelt Brian. “Als u ziek bent door een infectie of chirurgische ingreep, kunt u zich meer ‘off’ voelen omdat u medicijnen krijgt met een contra-indicatie voor uw eigen medicatie. Stress is ook een grote factor, die beslist een off-periode kan veroorzaken.
“Als je weet wat de oorzaak is, kun je die behandelen. Na een tijdje zijn ze weer terug op het niveau dat ze daarvoor hadden. Tenzij het met de medicatie verband houdt,” zegt hij.
Hij adviseert mensen met Parkinson om in een dagboek bij te houden wanneer ze off-periodes hebben, hoelang het duurt voor hun medicijnen werken en hoelang hun off-periodes duren, zodat ze dit aan hun zorgverlener kunnen doorgeven. Mensen met deze aandoening moeten een situatie vermijden waarbij ze in totaal acht uur per dag in een off-periode zitten.
Ten slotte raadt Brian mensen met Parkinson aan om zich aan het patroon van hun off-periodes aan te passen.
“Sommige mensen voelen zich ‘s ochtends heel goed. Naarmate de dag vordert, gaan ze zich slechter (off) voelen en zijn ze ‘s avonds dyskinetisch; dat is hun patroon. “Andere mensen voelen zich ‘s ochtends juist heel slecht, en naarmate de dag en de avond vorderen, gaan ze zich veel beter voelen. Dus pas uw dag en uw levensstijl aan als u weet dat deze periodes volgens een bepaald patroon verlopen.”
Als de off-periodes echt voor problemen gaan zorgen, zegt hij: “Vraag uw zorgverlener om hulp, om u te helpen uw symptomen beter te beheren. We kunnen heel snel vaststellen wat er aan de hand is.”
Parkinson’s Europe deelt dit artikel uitsluitend ter informatie; het is geen weergave van de opvattingen van Parkinson’s Europe, en Parkinson’s Europe wil hiermee geen specifieke behandelingen, therapieën of producten promoten.
« La vérité, c’est que les phases OFF, c’est nul ! » s’emporte Gary Boyle, membre du Conseil de Parkinson’s Europe, chez qui la maladie a été diagnostiquée en 2011.
Une phase OFF de la maladie de Parkinson correspond à un moment où les médicaments contre la maladie de Parkinson ne font plus effet.
« Il s’agit d’un phénomène à la fois moteur et non moteur. Quel que soit leur profil moteur et leur profil non moteur, les patients peuvent donc subir une aggravation de ces symptômes », explique Brian Magennis, infirmier spécialisé à l’hôpital Mater de Dublin et membre du Conseil de Parkinson’s Europe. « Et lorsque les effets des médicaments s’atténuent, ils peuvent ressentir des symptômes non moteurs, comme un engourdissement, des picotements, une sensation particulière dans le ventre, une sensation d’agitation, d’irritabilité, de mauvaise humeur, des fourmillements, toutes sortes de symptômes étranges et impressionnants – et dès que la dose suivante fait effet, ces symptômes disparaissent. »
En règle générale, les phases OFF commencent à se produire quand une personne est atteinte de la maladie de Parkinson depuis une dizaine d’années. Et comme chaque personne ayant la maladie de Parkinson la ressent différemment, les caractéristiques de ces phases OFF varient aussi.
Gary nous explique à quoi ressemblent ses phases OFF : « Je commence à avoir les mains et les bras qui tremblent. Je deviens très lent. Je n’arrive plus vraiment à écrire. J’ai du mal à utiliser mon téléphone. Je me sens déprimé, nerveux. Je commence à me demander : « Quand la prochaine phase ON va-t-elle commencer ? » Les phases OFF impactent à peu près tout. »
Bien que les termes « ON » et « OFF » suggèrent un déclin brutal, une phase OFF peut correspondre à une détérioration plus progressive.
Des facteurs tels que l’environnement et le mode de vie (régime alimentaire, nutrition, exercice et sommeil), ou encore le moment de la journée, ont tous un impact sur l’état d’une personne pendant ses phases OFF. Celles-ci peuvent se produire aussi bien la nuit que dans la journée. Et elles peuvent aussi se déclencher de manière soudaine, et sans raison apparente.
« Les phases OFF soudaines sont assez rares, mais quand elles se produisent, c’est vraiment handicapant », explique Gary. « Je n’ai jamais eu de phase OFF de plus de quatre heures (c’est le pire des cas), mais cela m’arrive presque tous les six mois, et surtout quand je m’y attends le moins. »
Si vous subissez de manière soudaine, pendant quelques jours ou semaines, plus de phases OFF que d’habitude, il y a probablement une raison, selon Brian. Cette situation est généralement un revers temporaire et ne signifie pas nécessairement que votre maladie de Parkinson progresse. Mais il est important de consulter un professionnel de santé qui pourra vous aider à en identifier la cause.
Dans la plupart des cas, comme l’explique Brian, une augmentation brutale des phases OFF est due à l’une des 10 raisons suivantes :
Vous êtes constipé. Cela peut affecter l’absorption de vos médicaments contre la maladie de Parkinson et les rendre moins efficaces.
Vous êtes malade (vous avez une infection urinaire ou respiratoire, ou la grippe) ou vous vous rétablissez d’un acte chirurgical. Ces états exercent une tension sur le corps, ce qui peut provoquer une aggravation temporaire des symptômes.
Vous traversez une période de stress.
Vous êtes déshydraté. Cela peut réduire le volume sanguin et affecter l’absorption des médicaments.
Vous ne prenez pas vos médicaments au bon moment, ou votre traitement a changé.
Vous prenez un médicament contre-indiqué pour un problème de santé non lié à la maladie de Parkinson, et cela affecte l’efficacité de votre traitement contre la maladie de Parkinson.
Vous êtes déprimé. La dépression peut provoquer une aggravation soudaine des symptômes moteurs et non moteurs.
Vous souffrez de douleurs aiguës ou chroniques.
Vous éprouvez de l’angoisse ou faites des crises de panique. Cela peut entraîner une augmentation des symptômes moteurs. L’angoisse est également un symptôme fréquent de l’épuisement de l’effet thérapeutique de la lévodopa en fin de dose.
Vous ne dormez pas bien. Une longue période de mauvais sommeil peut altérer (temporairement) la fonction motrice.
« La constipation est une cause importante parce qu’elle bloque l’absorption de la lévodopa », explique Brian. « Après une intervention chirurgicale, ou si vous êtes malade suite à une infection, il est possible que vous ayez plus de phases OFF après avoir pris certains médicaments contre-indiqués. Le stress est également l’une des causes les plus courantes de phases OFF.
« Une fois que vous avez identifié et traité la cause, il suffit d’attendre un peu pour que les effets reviennent à ce qu’ils étaient à la base. À moins que les symptômes ne soient liés aux médicaments. »
Brian conseille aux personnes atteintes de la maladie de Parkinson de tenir un journal de leurs phases OFF, en notant combien de temps leurs médicaments ont mis à agir et quelle a été la durée de leurs effets, afin de le montrer à leur professionnel de santé. Les personnes atteintes de la maladie de Parkinson devraient éviter de rester dans une situation où leurs phases OFF atteignent une durée totale de huit heures sur une journée.
Enfin, Brian conseille aux malades de Parkinson de s’adapter au rythme de leurs phases OFF.
« Certaines personnes se sentent vraiment bien le matin, puis fatiguent au fur et à mesure de la journée et sont plus en phase OFF et dyskinétiques le soir, et c’est leur rythme. D’autres se sentent vraiment mal le matin, et de mieux en mieux au fur et à mesure de la journée et jusque dans la soirée. Alors, si vous connaissez votre rythme, adaptez votre journée et votre style de vie en conséquence. »
Et si les phases OFF deviennent problématiques : « Allez voir votre professionnel de santé afin qu’il vous aide à mieux les gérer. Nous pouvons identifier ce qui se passe très rapidement. »
Parkinson’s Europe partage cet article à titre informatif seulement ; il n’est pas représentatif du point de vue de Parkinson’s Europe ni de son approbation de traitements, thérapies ou produits particuliers.
Eine OFF-Phase tritt ein, wenn die Wirkung von Parkinson-Medikamenten nachlässt.
„Es ist sowohl ein motorisches als auch ein nicht-motorisches Phänomen. Unabhängig vom motorischen und nicht-motorischen Profil eines Menschen können sich diese Symptome verschärfen“, erklärt Brian Magennis, Advanced Nurse Practitioner am Mater Hospital in Dublin und Vorstandsmitglied von Parkinson‘s Europe. „Und mittendrin, während das OFF-Phänomen beginnt, können nicht-motorische Symptome wie Taubheitsgefühl, Kribbeln, ein seltsames Bauchgefühl, Unruhe, Reizbarkeit, Übellaunigkeit oder Ameisenlaufen auftreten – alle möglichen befremdlichen Symptome. Und sobald die Wirkung der nächsten Dosis einsetzt, verschwinden diese wieder.“
Im Allgemeinen beginnen OFF-Phasen rund zehn Jahre nach dem Beginn der Parkinson-Krankheit. In einigen Fällen können sie bereits 4 bis 6 Jahre nach der Diagnose auftreten. Und ebenso wie jeder Mensch mit Parkinson die Erkrankung anders erlebt, unterscheiden sich auch die Merkmale der OFF-Phasen.
Gary Boyle berichtet, wie seine OFF-Phasen aussehen: „Meine Hand und mein Arm beginnen zu zittern. Ich werde sehr langsam. Ich kann nicht mehr schreiben. Es fällt mir schwer, mein Telefon zu benutzen. Ich bin deprimiert, nervös. Ich frage mich: Wann kehre ich in die ON-Phase zurück? Die OFF-Phase wirkt sich sowohl auf motorische, als auch auf nichtmotorische Symptome aus.“
Obwohl die Begriffe ON und OFF – also AN und AUS – eine rapide Verschlechterung nahelegen, kann die OFF-Phase auch graduell eintreten.
Faktoren wie Umwelt und Lebensweise – Ernährung, körperliche Aktivität und Schlaf – und die Tageszeit wirken sich auf die OFF-Phase aus. OFF-Phasen können nicht nur tagsüber auftreten, sondern auch nachts. Und sie können auch ganz plötzlich einsetzen – ohne offensichtlichen Grund.
„Plötzliche OFF-Phasen sind recht selten, aber wenn sie eintreten, sind sie eine enorme Behinderung“, sagt Gary Boyle. „Meine OFF-Phasen waren bisher nie länger als vier Stunden – das ist der schlimmste Fall –, aber das passiert fast alle sechs Monate, und zwar immer dann, wenn man es am wenigsten erwartet.“
Wenn plötzlich – innerhalb weniger Tage oder Wochen – mehr OFF-Phasen als üblich auftreten, gibt es wahrscheinlich einen Grund dafür, betont Brian Magennis. Diese Situation ist normalerweise ein vorübergehender Rückschlag und bedeutet nicht unbedingt, dass die Parkinson-Krankheit voranschreitet. Aber es ist wichtig, medizinischen Rat einzuholen, um die Ursache zu ermitteln.
In den meisten Fällen ist eine plötzliche Zunahme von OFF-Phasen auf einen von zehn Gründen zurückzuführen, so Brian Magennis:
Sie sind erkrankt (zum Beispiel an einer Harnwegs- oder Atemwegsinfektion oder an Grippe) oder Sie haben einen chirurgischen Eingriff hinter sich. Diese Faktoren belasten den Körper und können zu einer zeitweiligen Verschlechterung der Symptome führen.
Sie leiden an akuten oder chronischen Schmerzen.
Sie sind dehydriert. Dies kann das Blutvolumen reduzieren und sich auf die Resorption von Medikamenten auswirken.
Sie haben Verstopfung. Dies kann die Resorption von Parkinson-Medikamenten beeinflussen und ihre Wirkung beeinträchtigen.
Sie nehmen Ihre Medikamente nicht zum richtigen Zeitpunkt ein, oder Ihr Medikationsschema hat sich geändert.
Sie nehmen ein kontraindiziertes Arzneimittel für ein nicht Parkinson-bezogenes Gesundheitsproblem ein, das die Wirksamkeit Ihres Parkinson-Medikaments beeinträchtigt.
Sie stehen momentan unter starkem Stress.
Sie schlafen schlecht. Schlafstörungen über einen längeren Zeitraum hinweg können die Motorik – zeitweilig – beeinträchtigen.
Sie leiden an Angstzuständen oder Panikattacken. Dies kann zu einer Zunahme der motorischen Symptome führen. Angstzustände sind auch ein häufiges Symptom, wenn die Wirkung einer Levodopa-Dosis abklingt.
Sie sind depressiv. Dies kann zu einer plötzlichen Verschlimmerung sowohl der motorischen als auch der nicht motorischen Symptome führen.
„Verstopfung ist ein wichtiger Faktor, weil sie die Resorption von Levodopa blockiert“, so Brian Magennis. „Und bei einer Infektionserkrankung oder nach einem chirurgischen Eingriff sind OFF-Phasen häufiger, denn Sie sind möglicherweise mit kontraindizierten Arzneimitteln behandelt worden. Auch Stress ist ein wichtiger Auslöser von OFF-Phasen.
Sobald die Ursache ermittelt und behandelt wurde und ein wenig Zeit vergangen ist, erreichen die Betroffenen wieder ihren Ausgangszustand. Es sei denn, die Probleme sind medikamentös bedingt“, sagt Magennis.
Er empfiehlt Menschen mit Parkinson, Tagebuch über ihre OFF-Phasen zu führen und aufzuzeichnen, wie lange es dauert, bis ihre Medikamente wirken, und wie lange die Wirkung anhält. Diese Informationen können dann mit dem Arzt, der die Parkinson Krankheit behandelt, besprochen werden. Menschen mit der Parkinson-Erkrankung sollten Situationen vermeiden, in denen sie beispielsweise insgesamt acht Stunden am Tag eine OFF-Phase durchlaufen.
Abschließend rät Brian Magennis Parkinson-Patientinnen und -Patienten, sich auf das Muster ihrer OFF-Phasen einzustellen.
„Manchen Patienten geht es morgens sehr gut, aber das nimmt im Laufe des Tages ab und abends sind sie in einer OFF-Phase mit stärkeren Bewegungsstörungen. Das ist ihr Muster. Andere sind morgens stark beeinträchtigt, aber im Laufe des Tages nehmen die Symptome ab und abends geht es ihnen viel besser. Wenn Sie also wissen, dass ein Muster vorliegt, sollten Sie Ihren Tagesablauf und Ihre Lebensweise darauf einstellen.“
Wenn OFF-Phasen zum Problem werden, rät er: „Ihre behandelder Arzt kann Ihnen helfen, die Krankheit besser zu managen.“
Parkinson’s Europe veröffentlicht diesen Artikel ausschließlich zu Informationszwecken; er repräsentiert nicht die Ansichten von Parkinson’s Europe und stellt keinerlei Unterstützung für bestimmte Behandlungen, Therapien oder Produkte seitens Parkinson’s Europe dar.
Los periodos OFF en la enfermedad de Parkinson se producen cuando disminuye el efecto de la medicación.
«Se trata de un trastorno a nivel motor y no motor, así que, independientemente de cómo sea el perfil motor y laíndole del paciente, los síntomas pueden empeorar», explica Brian Magennis, enfermero especializado en el Mater Hospital de Dublín y miembro de la Junta de Parkinson’s Europe. «En plena crisis, cuando el tratamiento va dejando de hacer efecto, pueden aparecer síntomas no motores como entumecimiento, hormigueo, malestar estomacal, agitación, irritabilidad, mal humor, hormigueo… Todo tipo de síntomas raros y peculiares que luego, en cuanto la siguiente dosis hace efecto, desaparecen».
En términos generales, los episodios OFF comienzan a producirse cuando la persona lleva padeciendo Párkinson alrededor de diez años. En algunos casos, pueden ocurrir entre 4 y 6 años después del diagnóstico. Del mismo modo que cada persona con Párkinson experimentará la enfermedad de forma diferente, las características de sus periodos OFF también variarán.
Gary explica cómo son sus episodios OFF. «Me empieza a temblar la mano y el brazo. Voy muy lento. No puedo escribir bien. Me cuesta usar el teléfono. Me noto alicaído y nervioso. Empiezo a preguntarme cuándo volveré a la fase ON. El episodio OFF afecta prácticamente a todo».
Aunque los términos «ON» y «OFF» sugieren una empeoramento repentino, el paso al estado OFF se asemeja más a un deterioro gradual.
Algunos factores, entre los que se incluyen el entorno, el estilo de vida (como la dieta, la nutrición, el ejercicio y el sueño) y la hora del día, influyen en el estado OFF del paciente. Los episodios OFF pueden producirse tanto de noche como de día. Y también pueden aparecer de repente, aparentemente sin ningún motivo.
«Los periodos OFF repentinos son bastante raros, pero, cuando se producen, son muy debilitantes», afirma Gary. «Nunca he tenido un episodio OFF de más de cuatro horas, en el peor de los casos, pero me ocurre cada seis meses aproximadamente y cuando menos me lo espero».
Brian puntualiza que cuando, de repente, durante algunos días o semanas, experimenta más periodos OFF de las habituales, es muy probable que haya un motivo. Esta situación normalmente constituye un retroceso temporal y no significa necesariamente que el párkinson esté avanzando. Pero es importante consultar a un profesional sanitario para que ayude a identificar la causa.
En la mayoría de los casos, un aumento repentino de los periodos OFF se debe a alguno de los siguientes 10 motivos, explica Brian:
Enfermedad como, por ejemplo, alguna infección urinaria, respiratoria o una gripe, o la convalecencia tras una intervención quirúrgica. Estas situaciones estresan el organismo y pueden provocar un empeoramiento temporal de los síntomas.
Dolor agudo o crónico.
Deshidratación. Puede reducir la volemia y afectar a la absorción de la medicación.
Estreñimiento. Puede afectar a la absorción de la medicación para el párkinson y reducir su efectividad.
No tomar la medicación a las horas correctas, o cambiar el régimen de medicación.
Tomar un fármaco contraindicado para algún problema de salud no relacionado con el párkinson que hace que la medicación para esta enfermedad sea menos efectiva.
Periodos de estrés.
Falta de sueño. Un periodo prolongado de de insomnio o trastornos del sueño puede afectar, temporalmente, a la función motora.
Ataques de ansiedad o de pánico. Pueden ocasionar un aumento de los síntomas motores. La ansiedad también es un síntoma frecuente de que la dosis de levodopa está dejando de hacer efecto.
Depresión. Puede provocar un empeoramiento abrupto de los síntomas tanto motores como no motores.
«El estreñimiento es una de las más importantes, porque afecta a la absorción de levodopa», afirma Brian. «Si el paciente padece una infección o se somete a una intervención quirúrgica, es posible que tenga más episodios OFF, porque puede haber tomado alguna medicación contraindicada. El estrés es un factor importante que puede inducir periodos OFF.
«Cuando se identifica la causa, hay que tratar y esperar a que la situación se reestablezca. Todo vuelve al punto de partida. A menos que esté relacionado con la medicación», puntualiza.
Brian aconseja a las personas con párkinson que lleven un diario de sus periodos OFF y registren cuánto tarda la medicación en hacer efecto y cuánto dura, para poder informar a su médico. Las personas con esta enfermedad deberían evitar situaciones en las que pasan un total de, digamos, ocho horas al día en estado OFF.
Por último, Brian aconseja trabajar en el patrón de los episodios OFF.
«Algunas personas se encuentran muy bien por la mañana y, a medida que avanza el día, van empeorando y sintiendo más discinesia al atardecer; ese es su patrón. Otras se levantan muy mal y van mejorando mucho a medida que avanza el día. Por tanto, si se conoce el patrón, conviene programar el día y llevar un estilo de vida acorde con él».
Si los episodios OFF se convierten en un problema, explica: «Es necesario recurrir a nuestro médico para que nos ayude a gestionar mejor las cosas.».
Parkinson’s Europe comparte este artículo solo con fines informativos; no representa su punto de vista ni supone ninguna propuesta de ningún tratamiento, terapia ni producto en especial por su parte.
Un periodo OFF si verifica quando diminuisce gradualmente l’effetto del farmaco per il Parkinson.
“È un fenomeno sia motorio sia non motorio per cui, a prescindere dal quadro motorio e non motorio, si può verificare un peggioramento dei sintomi”, ha spiegato Brian Magennis, Infermiere specializzato presso l’ospedale Mater Hospital di Dublino, nonché Membro del Consiglio Direttivo di Parkinson’s Europe. “E poi, in questi episodi di passaggio allo stato OFF, possono subentrare sintomi non motori, ad esempio intorpidimento, prurito, uno strano fastidio allo stomaco, agitazione, irritabilità, scontrosità, formicolio: tutta una serie di sintomi strani e incredibili che, appena fa effetto la dose successiva, scompaiono”.
Generalmente, i periodi OFF iniziano a verificarsi quando una persona soffre di Parkinson da una decina di anni. In alcuni casi, possono verificarsi già da 4 a 6 anni dopo la diagnosi. Proprio come avviene con la malattia, che si manifesta in modo diverso da persona a persona, anche le caratteristiche dei periodi OFF variano.
Gary ci ha offerto la sua testimonianza. “Il primo sintomo a comparire è il tremore alla mano e al braccio. Mi muovo con grande lentezza. Non riesco a scrivere. Ho difficoltà a usare il telefono. Mi sento giù, nervoso. Inizio a chiedermi quando inizierà di nuovo una fase ON. Lo stato OFF incide praticamente su tutto”.
Sebbene i termini “ON” e “OFF” facciano pensare a un peggioramento repentino, il passaggio allo stato OFF tende a manifestarsi come un deterioramento graduale.
Sullo stato OFF di una persona incidono vari fattori, tra cui l’ambiente, lo stile di vita (regime dietetico, nutrizione, esercizio fisico e sonno) e il momento della giornata. I periodi OFF possono presentarsi di notte così come nel corso della giornata. E poi, possono insorgere all’improvviso, senza alcun motivo apparente.
“I periodi OFF improvvisi sono piuttosto rari, ma quando si verificano sono davvero debilitanti” ci ha raccontato Gary. “Non mi è mai capitato che un periodo OFF durasse più di quattro ore (questo è il peggiore dei casi che abbia vissuto), ma questi episodi si ripetono con una frequenza quasi semestrale e accadono quando meno te lo aspetti”.
Brian ha sottolineato che, se all’improvviso (nell’arco di pochi giorni o poche settimane) si verificano più periodi OFF del solito, probabilmente c’è un motivo. Di solito si tratta di una situazione temporanea, che non necessariamente indica una progressione del Parkinson. È comunque importante rivolgersi a un medico per risalire alla causa.
Brian ha precisato che, nella maggior parte dei casi, un aumento improvviso dei periodi OFF è dovuto a una di queste dieci cause:
Non stai bene (ad esempio, hai un’infezione urinaria o toracica o l’influenza), oppure sei in fase di recupero post-operatorio. Tali condizioni mettono a dura prova l’organismo e ne può conseguire un peggioramento temporaneo dei sintomi.
Soffri di un dolore acuto o cronico.
Il tuo corpo è disidratato. Tale condizione può ridurre il volume del sangue e influire sull’assorbimento del farmaco.
Soffri di stipsi. Tale condizione può influire sull’assorbimento del farmaco per il Parkinson e ridurne l’efficacia.
Non stai assumendo il farmaco agli orari corretti, oppure il tuo regime farmacologico è cambiato.
Stai assumendo un farmaco controindicato per un problema di salute diverso dal Parkinson e tale terapia sta riducendo l’efficacia del farmaco per il Parkinson.
Stai attraversando un periodo stressante.
Non dormi bene. Un periodo prolungato di insonnia o sonno disturbato può pregiudicare (temporaneamente) la funzionalità motori
Soffri di ansia o attacchi di panico. Tali stati possono determinare un aumento dei sintomi motori. L’ansia rappresenta anche un sintomo frequente della riduzione dell’efficacia di levodopa, chiamata effetto di wearing off, o di fine dose.
Soffri di depressione. Tale condizione può causare un peggioramento improvviso dei sintomi sia motori sia non motori.
“La stipsi incide notevolmente, perché compromette l’assorbimento di levodopa” ha chiarito Brian. “Se hai contratto un’infezione o hai subito un intervento chirurgico, potresti andare incontro a fasi di OFF più intense, perché potresti dover assumere alcuni farmaci controindicati. Lo stress è un fattore importante, che incide notevolmente sull’insorgere delle fasi OFF”.
“Una volta identificata la causa, bisogna trattarla e attendere: la situazione si ristabilizzerà. A meno che sia correlata al farmaco”, ha aggiunto.
Brian consiglia alle persone con la malattia di Parkinson di tenere un diario dei periodi OFF da mostrare al proprio medico, in cui annotare il tempo necessario perché i farmaci abbiano effetto e la durata dell’efficacia. Le persone con questa malattia devono cercare di evitare situazioni di notevole disagio, come avviene se ci si trova in fase OFF per otto ore al giorno.
Infine, Brian consiglia alle persone con il Parkinson di modificare la propria routine in funzione dell’andamento dei propri periodi OFF.
“Alcune persone al mattino stanno bene; poi, col passare delle ore, l’effetto del farmaco diminuisce e verso sera subentra la fase OFF e si accentua la discinesia: questo è il loro pattern. Altre persone stanno molto male al mattino e col passare delle ore e l’avvicinarsi della sera, stanno molto meglio. Quindi, se si riconosce la presenza di uno schema ricorrente, è opportuno adattare la propria giornata e il proprio stile di vita di conseguenza”.
Se i periodi OFF diventano difficilmente tollerabili, la raccomandazione di Brian è: “Consultate il vostro medico perché vi aiuti a gestire meglio la situazione.”.
Questo articolo è stato distribuito da Parkinson’s Europe unicamente a fini informativi; il testo non riflette le opinioni di Parkinson’s Europe e non costituisce un avallo da parte di Parkinson’s Europe di specifici trattamenti, terapie o prodotti.
“A realidade dos episódios OFF é que são muito desagradáveis”, afirma Gary Boyle, membro da direção da Parkinson’s Europe, a quem foi diagnosticada a doença de Parkinson em 2011.
Um episódio OFF é o que acontece quando a medicação para a doença de Parkinson começa a perder efeito.
“É um fenómeno motor e não motor e, como tal, qualquer que seja o seu perfil, , pode haver um agravamento desses sintomas”, explica Brian Magennis, Enfermeiro Especialista no Mater Hospital em Dublin e membro da direção da Parkinson’s Europe. “Nos episódios OFF, podem ocorrer sintomas não motores, como dormência, formigueiro, uma sensação estranha na barriga, agitação, irritabilidade, nervos, picadelas, vários sintomas estranhos e maravilhosos. E depois, quando a dose seguinte começa a fazer efeito, desaparecem.”
De um modo geral, os episódios OFF começam a surgir quando a pessoa tem Parkinson há cerca de dez anos. Em alguns casos, podem ocorrer 4 a 6 anos após o diagnóstico. Cada pessoa com Parkinson tem uma experiência diferente da doença e, do mesmo modo, as características dos episódios OFF também variam.
Gary explica como são os seus episódios OFF. “Começo a ter tremores na mão e no braço. Fico muito lento. Não consigo escrever. Tenho dificuldade em utilizar o telefone. Sinto-me em baixo, nervoso. Começo a pensar: quando é que vou voltar a estar ON? Estar OFF tem impacto em quase tudo.”
Embora as expressões ON e OFF sugiram um declínio acentuado, o OFF apresenta-se mais como uma deterioração gradual.
Fatores como o ambiente e o estilo de vida (dieta, nutrição, exercício e sono) e a hora do dia, podem ter impacto na manifestação do OFF de uma pessoa. Os episódios OFF podem ainda ocorrer tanto de dia como de noite. E podem acontecer de repente, sem motivo aparente.
“Os episódios OFF repentinos são bastante raros, mas, quando acontecem, são bastante debilitantes”, refere Gary. “Nunca estive OFF mais do que quatro horas, no pior dos casos, mas isso acontece quase de seis em seis meses e acontece quando menos se espera.”
“Se, de repente, ao longo de alguns dias ou semanas, estamos a ter mais episódios OFF do que o normal, é provável que exista um motivo”, explica Brian. Esta situação é habitualmente um contratempo temporário e pode não significar que a doença de Parkinson esteja a progredir. Contudo, é importante consultar um profissional de saúde que possa ajudar a identificar a causa.
Na maioria dos casos, um aumento súbito dos episódios OFF deve-se a uma de 10 razões, de acordo com Brian:
Doença (por exemplo, uma infeção urinária ou respiratória ou gripe) ou recuperação de uma cirurgia. São situações que colocam pressão no organismo, o que pode provocar um agravamento temporário dos sintomas.
Sofre de dor crônica ou aguda.
Desidratação. Pode reduzir o volume sanguíneo e afetar a absorção dos medicamentos.
Obstipação. Pode afetar a absorção da medicação para a doença de Parkinson e torná-la menos eficaz.
Não toma os medicamentos à hora certa ou o regime de medicação mudou.
Está a tomar um medicamento para um problema de saúde não relacionado com a doença de Parkinson que é contraindicado porque reduz a eficácia da medicação para esta doença.
Está a atravessar um período de stress.
Sono não reparador. Um período prolongado de sono insuficiente pode afetar temporariamente a função motora.
Ansiedade ou ataques de pânico. Pode acentuar os sintomas motores. A ansiedade é também um sintoma frequente de que a dose de Levodopa está a começar a perder efeito.
Depressão. Pode causar um agravamento súbito dos sintomas motores e não motores.
“A obstipação é um dos principais problemas, na medida em que bloqueia a absorção de Levodopa”, explica Brian. “Se estivermos doentes com uma infeção ou no seguimento de uma intervenção cirúrgica, podemos estar mais OFF, porque pode ter sido necessário tomar alguns medicamentos contraindicados ou foram realizadas alterações não planeadas na medicação habitual. O stress é um fator importante que pode mesmo despoletar um episódio OFF.”
“Depois de identificar a causa, tratar a causa e dar algum tempo, tudo volta ao ponto em que estava. A menos que seja uma questão relacionada com medicamentos”, diz.
Brian aconselha as pessoas com a doença de Parkinson a escreverem um diário dos seus episódios OFF, registando o tempo que os medicamentos demoram a fazer efeito e quanto tempo duram, para depois mostrar ao profissional de saúde. As pessoas com esta doença devem evitar situações em que, por exemplo, passem um total de oito horas por dia em estado OFF.
Por fim, Brian aconselha as pessoas com a doença de Parkinson a trabalharem com o padrão dos seus episódios OFF.
“Algumas pessoas funcionam muito bem de manhã e, à medida que o dia avança, vão-se desgastando e ficam mais OFF e discinéticas à noite. Outras pessoas sentem-se muito mal de manhã e, à medida que o dia avança e à noite, ficam muito melhores. Se conseguir identificar um padrão, adapte o seu dia e o seu estilo de vida nesse sentido.”
Segundo Brian, se os episódios OFF se tornarem problemáticos: “Consulte o seu profissional de saúde para gerir melhor a situaçâo.”.
A Parkinson’s Europe partilha este artigo apenas para fins informativos; não representa a opinião da Parkinson’s Europe e não constitui uma aprovação pela Parkinson’s Europe de quaisquer tratamentos, terapias ou produtos específicos.
We all know the benefits of daily exercise. Being active has such a positive impact on physical and mental health, often making you feel great both inside and out. People with Parkinson’s are around a third less active than other people of the same age. But the more active you are, the easier you will find it to manage your symptoms.
Whatever your fitness level, you can find the exercise that works best for you – whether that is a long countryside walk with friends or simple chair-based workouts at home. Making exercise part of your regular routine will lift your mood and help you keep your body moving more effectively.
Speaking to your physio or doctor for advice before starting any new exercise regime is worthwhile. They will be able to suggest the best kind of physical activity to start with.
Physiotherapist (and President of Parkinson’s Europe) Josefa Domingos – who has spent decades specialising in physiotherapy for Parkinson’s – has approved the following advice.
Tips on how to keep active and exercise effectively and safely with Parkinson’s
Reduce the amount of time you sit each day. For example by walking rather than driving short distances, getting off the bus one stop early or making a walk part of your daily routine. Where possible, take the stairs rather than a lift or escalator. It really does make a difference.
Try to exercise for at least 150 minutes each week. During each session you should aim to get warm, sweat lightly and be out of breath to the point that it is hard to keep up a conversation. How you make up the total time is up to you. However, it is better to exercise two or three times a week for shorter periods than just a long session at weekends. You could try five sessions of 30 minutes. If that is too long at once, then repetitions of two 15-minute periods or three bursts of 10 minutes each is also fine.
Make sure you include different styles of exercise. Aim for a range that will extend your endurance, build and maintain muscle strength, and maintain joint flexibility and your ability to stretch.
Improve your functional mobility. For example, try making large amplitude ranging movements with your arms and legs when you are sitting, lying down, standing or walking. These will help with daily activities such as walking and balance.
Enjoy. Exercise should be fun! So pick something you enjoy and which suits your daily life, physical capabilities and movement goals you want to achieve. You are far more likely to maintain your regime if you enjoy what you are doing, feel able to cope and help you improve!
Use the buddy system. An exercise ‘buddy’ or group sessions are great for moral support and motivation. Consider joining organised or group classes at your local gym or other public venues, particularly if they are Parkinson’s specific or provide recognised benefits for people with Parkinson’s such as dance,Tai Chi, pilates, boxing and others.
Choose your time. Try to exercise when medication is working well and you are feeling rested as movement will then be easier for you.
Know when to stop. It is normal to feel tired when exercising and a little after. The fatigue related to exercising should not last the rest of the day. During exercise remember to stop if anything hurts or feels uncomfortable. You should talk to your doctor if you experience any of the following when exercising:
pain
nausea
light-headedness
dizziness
a tight chest for more than a few minutes
or if you feel your heart missing or adding beats.
Listen to your body and learn to recognise when to stop.
Consult your doctor. If you have recently had a heart attack, have any other heart problems or have been told that you are at risk of heart disease then you should consult with your doctor before you embark on an exercise programme. You should also talk with your doctor before exercising if you have been inactive for a long time.
“It’s been a quiet miracle” Janette Sinclair on her DBS experience
Parkinson's Europe Board member Janette Sinclair tells us about her recent personal experience of Deep Brain Stimulation, which she underwent in January,2025.
Janette Sinclair is a UK national living in Brussels Belgium with her husband and son. She is a member of the Parkinson’s Europe Board. Here, she tells us about her recent personal experience of DBS (Deep Brain Stimulation surgery), which she underwent in January 2025.
“I was diagnosed with Parkinson’s in 2013, aged 50. For the first nine years, I managed quite well with a lot of exercise, and medications like Requip (ropinerol) and Azilect. I was not keen on levodopa, as it gave me highs and I found it unreliable. But then things started to get more complicated. I was no longer able to get the same results with agonists alone. I reluctantly started taking levodopa in the form of Stalevo and quickly ramped up to five times a day while still taking quite a large dose of Requip. I was also taking other medication like soluble and slow-release prolopa and Xadago.
I was having more and more difficulties with the unpredictability of the medication. In the end, I never knew when I was going to go off and this eroded my confidence to the point where I would not even feel comfortable walking five minutes to our local shops. I had always been very independent in the past and this was not only a physical challenge for me, but also a huge psychological battle. I think people looked at me and thought that I was in quite good shape but I just could not cope with the swings, four or five times every day, between ‘ons’ and ‘offs’, and the nights mostly ‘off’.
I really felt I had nowhere to go, and had even started thinking about assisted dying (which is legal in Belgium).
This was compounded by my work situation. I had managed to keep working at a relatively senior level, but the last year defeated me and I was off on sick leave for a year until I retired last November.
Making the decision to begin my DBS experience
“I was ‘in between’ neurologists due to departures at my local hospital and I therefore took advice from a British neurologist at King’s Hospital London. In fact I had seen him when I was first diagnosed with Parkinson’s and he had mentioned DBS as a solution, I even met the surgeon. But when I started looking into the practicalities, several years later, it was clear that it would be very complicated to have the operation in the UK while living in Belgium. So at the beginning of 2024, I started investigating DBS possibilities in Brussels and surroundings.
I was looking for an multidisciplinary team with lots of DBS experience, not so obvious in a small country like Belgium; and I wanted to have the operation done while asleep. I was terrified of the idea of being awake during part or all of the operation and I was already imagining every conceivable disaster scenario.
There was a sense of urgency around my search because there is a window of opportunity for DBS; it needs to be done while the body is still in reasonable shape, as posture changes cannot easily be reversed. I worried that chronic problems with my lower back and my neck would decline before I had the operation and cause problems.
The university hospital has a large Neurology department and specialises amongst other things in Parkinson’s with a DBS unit and a Parkinson’s nurse. We met the surgeon several times. He answered all my questions seriously and explained the risks, and I had a good feeling about him.
Up to then, I had been in exploration mode, but decision-time for me came in June 2024 when we were discussing the details of the operation – he said that he usually had the patient awake during at least part of the operation. I asked, “Could you do it with me asleep throughout?” He said that he could, citing some references that showed the benefits of awake versus asleep procedures, mentioning that he did similar operations asleep for other pathologies and referring to the fact that the robotics he used helped with the accuracy of the electrodes placement (the main reason for keeping the patient awake).
So I surprised everyone by signing up there and then. Once I had made up my mind, I asked for the earliest date possible, which turned out to be the beginning of January.
My experience begins: DBS assessments
“We discussed risks, the main ones being infection and bleeding on the brain. The hospital had a low incidence of both, however, when these occur they can be catastrophic. Each of us reacts differently to risk and each one will make his or her own decision. I tried to put things in perspective because the DBS procedure has been around for several decades now, and nowadays is a fairly routine and safe procedure.
Not everyone is suited for the operation, so there were some important and rigorous tests to go through before I could have the operation. The most important test is the levodopa challenge. Basically, a good response to levodopa is a good indicator for DBS success, so the doctors want to see how you react off levodopa, and then how good your response is when the medication is reintroduced. The test requires overnight hospitalisation in case there are difficulties or a bad reaction, and all I can say is that I was very grateful to my neurologist when he let me take my last dose of medication at 8pm – so the night was bearable – before stopping all of my medication.
The next morning, at around 10am, I was filmed while in an ‘off’ state – it was horrible, especially the mental shutdown. The neurology team checked the video – it was enough! – and I was allowed my medication. Once the meds kicked in, I was filmed again to show me doing the same exercises while fully ‘on’. I was told that, as a rule of thumb, at best the DBS might match my ‘on’ results, but was unlikely to be better. This was a good way for us to understand what I might achieve through the DBS experience, to manage expectations. I was happy, though, as I usually had very good results when my meds were working, they just didn’t work for long enough.
The other extremely important test is a Neuropsychiatric evaluation. Essentially, this is a whole barrage of cognitive tests aimed at assessing memory, to see if there is any risk or sign of dementia. The tests took around three hours. There was a questionnaire to assess emotional status. The cognitive tests were very varied and quite intense: naming images, remembering and repeating long lists of words, copying shapes and patterns. I personally really enjoyed it, but it was very tiring and I can imagine it could easily be very stressful for some people.
Pre-op nerves
“My operation date had been reserved and was now confirmed for 6 January – Epiphany, which seemed auspicious. I thought I felt fine about it, but with hindsight I was letting my anxiety get away from me, and I got really wound up about an administrative issue, regarding direct billing of costs of the operation to my health insurance. It was a low point for me, focusing intensely on one issue, writing long emails, avoiding the phone, spiralling (typical Parkinson’s?!)
Luckily everyone was very patient with me, and the issue was resolved quickly and positively.
Then suddenly it was Christmas and I started to have doubts. I felt that I did not know enough of what I was letting myself in for, not helped by my husband Carl who took the view that I had nothing to lose and plenty to gain, and according to him that was all I needed to know. I tried to find more specific practical information about the operation and what happens afterwards.
The hospital had quite a long and detailed guide to the DBS experience, but it was in Dutch and for (unknown) technical reasons we could not get it translated. But other reputable guides were available and they were all much of a muchness, with technical descriptions of process, how the device would work etc, but nothing really about what it would feel like, how long it would take for the wounds to heal, what the physio/exercise regime was like etc.
Was there someone I could talk to? I realised that I only knew a few people who had experienced the operation. They were happy to give me answers about their own DBS experience if I could just work out what questions to ask!
Just before my operation date, we spent the evening with friends. After about half an hour I went off my meds, and spent nearly two hours lying on the floor while waiting for the next dose to kick in. By the time I was feeling okay, it was already gone 11pm. Too late to enjoy the food, but we sat chatting. And then my meds went off again! I knew that if we did not leave immediately I would not manage the 10-minute walk home before the rigidity and slowness set in.
The couple we were visiting had experience of Parkinson’s and they were very sympathetic to my difficulties, but other people can be less understanding and even when people make the effort, I know that my own reaction is not neutral. I may have Parkinson’s but I still wanted to keep my dignity when the Parkinson’s was showing; I worried about being vulnerable in ‘unsafe’ places (which by now had become anywhere other than inside my own home); I hated looking ‘weird’ and drawing stares.
January loomed, cold and dark. I was scheduled to report to Leuven hospital on 4 January, but there were practical points that I still wanted to confirm before the surgery – which make of device I would have implanted, whether to have left or right-side placement of the neurostimulator, whether to choose a rechargeable device or not. Another long letter later, and once more I was reassured, this time with a detailed reply from the surgeon himself, addressing each point and proposing to pass by on the Sunday evening before the operation.
Just before the operation was due, we realised we had not signed a Power of Attorney allowing Carl to manage my health insurance affairs in the event that I was incapacitated. There were probably other things we should have done…
Janette and Carl at Christmas
My DBS surgery experience
“I checked into the hospital and settled into my room. When we arrived we were informed of a pilot project allowing a nominated person to stay for longer hours, beyond the regular visiting hours. We jumped at this opportunity, given my concerns about stopping my medication: from Sunday morning, no more Parkinson’s meds were allowed. I handed in the large pack of drugs I would usually take over 2-3 days, to avoid any temptations I might have to ease the ‘off’ time. As I got more and more ‘off’, I resorted to movement for relief, stretching out my back as much as possible.
Carl and I decided to do laps around the ward corridors, going slower and slower as the evening progressed. The surgeon came by at around 9pm and went through the basics of the operation. It was really good to see him, though I’m not sure how much I took in. Not for the first time, it flashed through my mind that I ought to record such conversations so I could listen to them later.
Carl was about to go home, planning to come back early in the morning. I was anticipating a difficult night, and on a whim, I asked if he could stay. The staff looked dubious and went off to investigate. To my surprise, the response was positive, and they made up a sofa bed straight away. I didn’t get much sleep throughout the night – my legs were spasming and twitchy – but at least I was not alone.
Next morning, it was dark and snowing outside. I got washed and was helped into a hospital gown. At around 7am we headed down to the operating theatre. Carl was allowed to come with me part of the way. He was evidently taking things very seriously, as his usual jokey patter had vanished.
Then I was on my own. UZ Leuven is a very large hospital and I realised that there were dozens of people on hospital beds being brought down to a central dispatching hub. Someone came and checked my name and asked which operation I was going to have (was there a choice?!), then I was off again to the end of the corridor. Once there, a series of medical staff came up to me and introduced themselves, promising to look after me during the operation. Then came the surgeon, and he wished me good luck!
Everyone was very busy getting organised, and then came the anaesthetist, who told me to countdown from ten: ’10, 9, 8…’
The next thing I knew, people were calling my name and trying to wake me. I was resisting, enjoying such a good sleep, but in the end I gave into the inevitable and opened my eyes. It was evening already. Apparently people with Parkinson’s take longer to come round after a general anaesthetic. My operation had finished early, by 1.30pm, but I did not come round till much later. Carl had gone home but was now back, having panicked when the surgeon rang early to tell him the operation was done.
My head was a mass of black stitches and congealed blood with dressings stuck on top. There were more things going on there than I had expected, for example the cable and connection behind my ear running down to the device. It had to go somewhere I suppose… But my hair was mostly intact and there was very little pain – just a slight headache, which soon passed.
The neurostimulator was not yet turned on, and I was disappointed to be put back on my pre-op levels of medication, even though I had expected this. I was not as dependent on them as before, however, due to the strange effect of brain swelling after the operation.
Post-surgery recovery and DBS device switch-on
“And two days later I was on my way home to heal. A largely uneventful few weeks followed, except for the joys of trying to remove a very sticky and tenacious substance from my hair while being mindful of the head wounds. The challenge was beyond me and I ended up cutting out the worst tangles from my hair.
Apparently the substance was silicone, placed onto the stitches to keep them clean, but impossible to remove with shampoo. I also had a little scare when the wound behind my ear looked a bit red and infected. I called the DBS Secrétariat, sent photos, and spoke directly with the surgeon, who immediately asked me to come in for a check-up straight away, which I was happy to do. We were both relieved when he gave the ‘all clear’.
In the period from 8 January to 9 February I generally felt well, though tired, and I looked well and was able to do some exercise. I was still taking my full meds but did not feel the same desperate reliance on them that I felt before the operation, although the effect had finally worn off by the beginning of February.
On Sunday 9 February, it was back to Leuven, checking into the Neurology ward again. Carl took advantage of the extended visiting hours again but could not stay overnight as this time I was sharing a room with another DBS patient. He hung around as long as he could before heading home, leaving me to face a difficult night – yet again, I had to stop taking all my meds, this time so that an ‘OFF’ baseline could be established before setting the device.
First thing the next morning the DBS expert, Dr Swinnen, arrived and took me off for baseline testing of my neurostimulator device.
He began by running through various programmes to establish some guide measurements. I reacted quite strongly to the higher levels each time – I felt that the skin around my eyes was tingling and pulling tight, which was very unpleasant. Once this was done we fixed the setting quite low, and I was prescribed 8mg of Requip and 2 prolopa 250 tablets.
There was no “Eureka!” moment for me: the device just took the place of the drugs I had been taking, only it worked all the time, with no dosage fails or nighttime panics. A quiet miracle.
The aim when regulating the device is to find the best mix between the device settings and the medication, as measured by the levels of dyskinesia and ‘off’ states. For the next two days the device was gradually adjusted, and my reactions were closely monitored. Then, my levodopa dosage was reduced to 1 tablet per day.
Over the next four months, I have had regular appointments with the team to regulate the neurostimulator device – twice weekly the first two times, then weekly, and then with a gap of a fortnight and a month to accommodate my holidays. At each visit, a detailed record of my everyday symptoms and reactions were taken and discussed, and we then agreed what action to take – most often, we would increase the settings of the device by a few points, as I was more susceptible to ‘off’ symptoms than dyskinesia.
We, or rather, Carl did the adjustments, each time we had clear parameters for the changes. We went to Wales to visit my mother. She was so pleased to see the changes in my condition.
I did not manage to sustain my fitness levels after the operation and so I organised a 4-week physical rehab programme at a specialist centre in Portugal, called Centro Neurologico Senior, in Torres Vedras.
A pile of Janette’s now-redundant Parkinson’s medication!
Four months on: reflections from my DBS experience
“It’s important to emphasise that four months on from the operation, my body is still gently healing, and I am still going through the initial phase of adjustment of the neurostimulator.
But let me just say that I’m really happy the way things are going. I didn’t have a dramatic moment when the neurostimulator was first turned on – I’m told that is more likely to happen for tremor-dominant patients, whereas I had more rigidity.
For me, it’s been more of a quiet miracle – my DBS device works 24/7, and without the drugs.
In fact, l have reduced the levodopa I was taking by around 80%, the agonist Requip by nearly half, and I have stopped just about everything else.
The downsides of my DBS experience
“There are a few things on the negative side, but so far they seem to be manageable :
The extension wires in my neck connecting the neurostimulator to the brain are a bit tight – I’m doing physio as advised, and will see the surgeon later if there is no improvement.
I’ve put on weight – around 10 kilos. This seems to be a fairly common response following DBS.
The charging pack is heavy and not very user-friendly.
There were also a few things missing from my DBS experience which, on reflection, would have been helpful:
Written guidance on scalp wound care, covering:
The location of wounds
Stitches care and removal
How soon I can wash and/or dye my hair
Any special products I could use, for instance to remove the silicon from my hair
Scar treatment
How long sensitivity / pain/ numbness would last
Advice on regular/ routine tests to get out of way before the operation, for instance a mammogram
Advice on weight gain – if I’d been more aware, would have made an effort to stem the excess eating
More information on the sheer physicality of neurotransmitter – not comfortable for me. A problem affecting women more than men?
User-friendly guidance on things to avoid for battery safety, such as saunas, sunbathing, swimming, and different types of medical scans and imagery
Despite the substantial progress so far, I believe that my DBS adventure will be continuing for a long time yet, and I’m looking forward to the new lease of life it has given me.
What does my DBS experience mean in practice?
“I’m gradually regaining my confidence to go out by myself, and this means I am regaining my independence – I started by walking to the local shops 10 minutes away, and then staying out for longer each time. Recently, I went alone to a World Parkinson’s Day event – a journey of around 30 minutes on public transport and a 10-minute walk at each end – and finished the day with dinner with friends.
This is nothing and everything: most of you do this every day, but those of you familiar with more advanced Parkinson’s will know what I’m talking about.
I can go to bed without fear.
I can use chopsticks again.
And my husband said he got me back.”
Note: Janette was treated at UZ Leuven under the care of neurologist Professor Dr Wim Vandenberghe, neurosurgeon Professor Dr Philippe De Vloo, and Dr Bart Swinnen, a neurologist specialising in DBS.
Discover more DBS experience stories in our Demystifying DBS campaign, including Ivan’s DBS experience in Ireland in our in-depth article, and Gerlach Roomans’ DBS experience in the Netherlands in our DBS podcast.