
Three experts share how deep brain stimulation (DBS) visualisation software is revolutionising treatment for people with Parkinson’s disease
Deep brain stimulation is an established treatment for people with Parkinson’s disease, but industry experts think that its fast evolution has led to an information gap. This means that those who may benefit from the technology may not be aware of all the latest innovations – and how these new developments in the field could be of benefit to themselves, friends or family members.
DBS treatment involves the placement of two electrodes into the brain, which then deliver electrical impulses through a connected stimulator. Targeting specific regions of the brain, the impulses can improve Parkinson’s symptoms by blocking certain signals and helping to improve uncontrolled muscle movements.
Professor Jens Volkmann, who heads a team at the University of Würzburg, Germany, says: “The impact of DBS is all about location”. That’s why, when it comes to placing these electrodes, clear visualisation of the tech’s inner workings could offer a step forward in Parkinson’s treatment.
Older versions of programming software offered limited information on the location of simulated DBS leads. But working with new software, like Boston Scientific’s new GUIDE-XT – which uses information from individual patient MRI and CT scans to create a 3D visualisation of the leads in relation to the brain – has helped neurologists like Professor Volkmann to improve quality control and reduce the time required for programming.
In fact, says his fellow researcher Dr Martin Reich, “Visualisation software will change the way we programme patients in the future”.
Visualising the benefits of DBS
Discussing the potential benefits of DBS visualisation, Professor Volkmann says: “In a way, it is like GPS or Google Maps: it helps us to orient ourselves in 3D space”.
Patient-specific ‘maps’ highlight the targeted area for stimulation, as well as surrounding anatomy – without which healthcare professionals rely on trial and error to locate the best electrode location for each patient.
“You need to know exactly which few cubic millimetres of tissue in a certain area need to be stimulated, to produce the best possible effects and to avoid adverse effects,” says Professor Volkmann. “The visualisation software is helping us to track the areas that are influenced by a certain electrical field.”
He adds that the software means that the time spent “troubleshooting” in the clinic is reduced.
“In the past, I needed to test patients,” says Dr Philipp Capetian, senior consultant and head of the university’s DBS outpatient clinic. “You would programme what you thought you needed and wait. But now you really know where the electrodes are located, and you can simulate the currents and see the field you can achieve with stimulation. You know your target structure, the electrodes in relation to that and where your contact is located.”
Making an “educated choice”
Some people with Parkinson’s may be hesitant about DBS. Not only is it a surgical procedure, but it could also lead to adverse effects if electrodes are not positioned optimally in the brain or programmed effectively.
But with new developments in the field, many people with Parkinson’s can approach DBS with greater confidence. For Dr Reich and some of his patients, this could be a “game-changer”.

“Let’s say a patient with Parkinson’s disease has gait-freezing,” adds Professor Volkmann. “The first thing we want to know is where the electrode is located. Is it on target? Are we overstimulating the target? Before we had visual programming, we would do a blind flight – changing parameters following certain clinical algorithms, trying different options for two or three weeks.
“We can accelerate that now. We can look at the images and make an educated choice. That is the big difference – this is much more likely to get to a good clinical solution, in a much shorter time.
“We have patients now who have had DBS for years and have particular problems. We can perform an image-based review of their electrode position and programming options, and continue to come up with improvements.”
“An era of digital revolution”
Data gathered through the DBS process could also help patients in the future, says Dr Reich. The hope is that artificial intelligence approaches – “collecting many already-operated patients and analysing them” – will help inform settings used for individual patients in programming.
Professor Volkmann agrees: “We are in an era of digital revolution. Once we have the data available, the visualisation software will allow us to pool data from different centres because we have a common reference.
“That could be a very interesting approach for image analysis. You learn on an individual basis from the one patient in your big database and compare this to the patient that you are currently programming.”
A clearer picture of the needs that exist for people with Parkinson’s could then help to inform treatment – and offer more personalised care in the future.
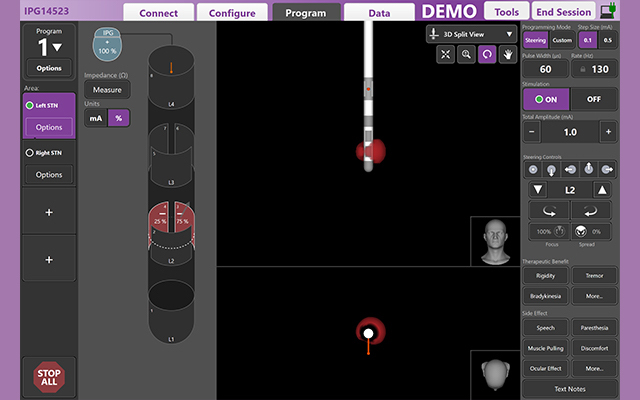
Lead image: Visualisation software Guide-XT from Boston Scientific, which uses 3D-imaging of patient-specific anatomy to help with programming.
Parkinson’s Europe is sharing this article for information purposes only; it does not represent Parkinson’s Europe’s views and is not an endorsement by Parkinson’s Europe of any particular treatments, therapies or products.


